Extensor Mechanism Injuries
Patellar & Quadriceps Tendon Tears
The quadriceps tendon (above the kneecap) and the patellar tendon (below the kneecap) are the powerful tendons that allow you to straighten your knee. A rupture of either tendon is a serious injury that usually requires surgical repair to restore the ability to straighten the leg, walk and return to activity.
How they occur
These tendons most commonly tear during a sudden, forceful contraction of the thigh muscle against a bent knee — for example landing awkwardly, a stumble or fall, or lifting a heavy load. Patellar tendon ruptures tend to occur in younger, active people, while quadriceps tendon ruptures are more common over the age of 40. Pre-existing tendon weakness from previous injury, steroid use or certain medical conditions can increase the risk.
Symptoms
Most patients feel a sudden pop or tearing sensation at the front of the knee, followed by pain, swelling and bruising. The hallmark is an inability to straighten the knee or to keep it straight when lifting the leg. There is often a palpable gap above or below the kneecap, and the kneecap may sit too high (with a patellar tendon tear) or too low (with a quadriceps tendon tear).
Diagnosis
The diagnosis is usually clear from the history and examination. X-rays show the position of the kneecap and can help confirm the injury, while ultrasound or MRI confirms the tear, shows whether it is partial or complete and helps plan the repair.
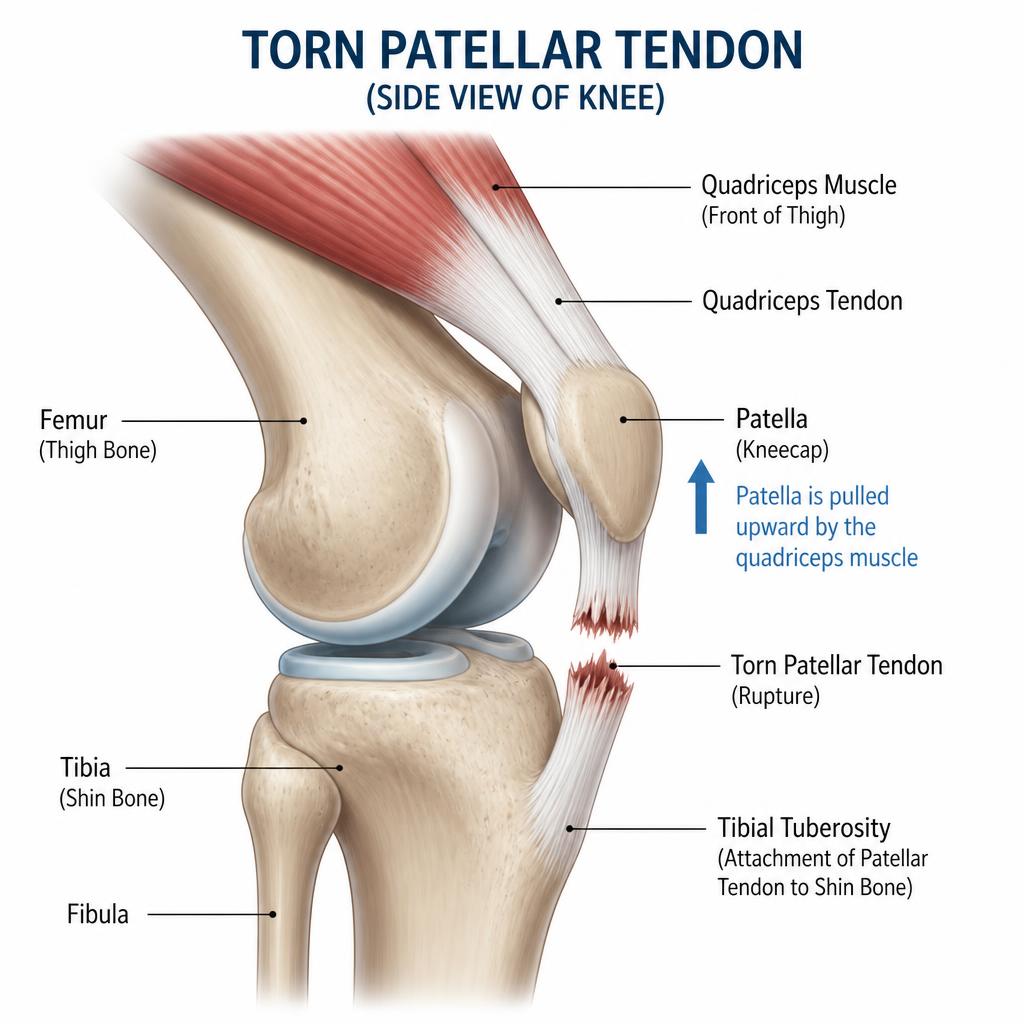
Patellar tendon tear
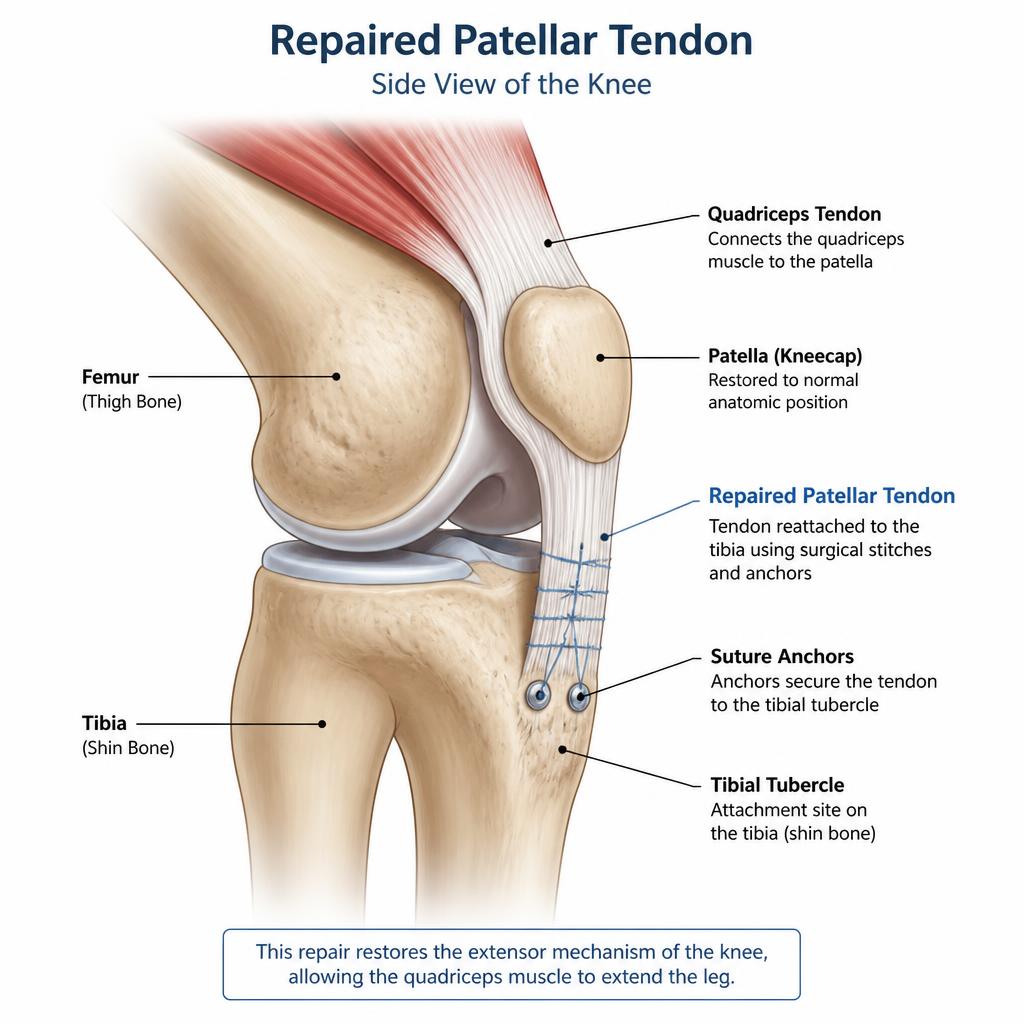
The patellar tendon connects the kneecap to the shin bone. When it ruptures, the kneecap is pulled upwards and the knee cannot be straightened. The images below show the injured tendon and the tendon after surgical repair.
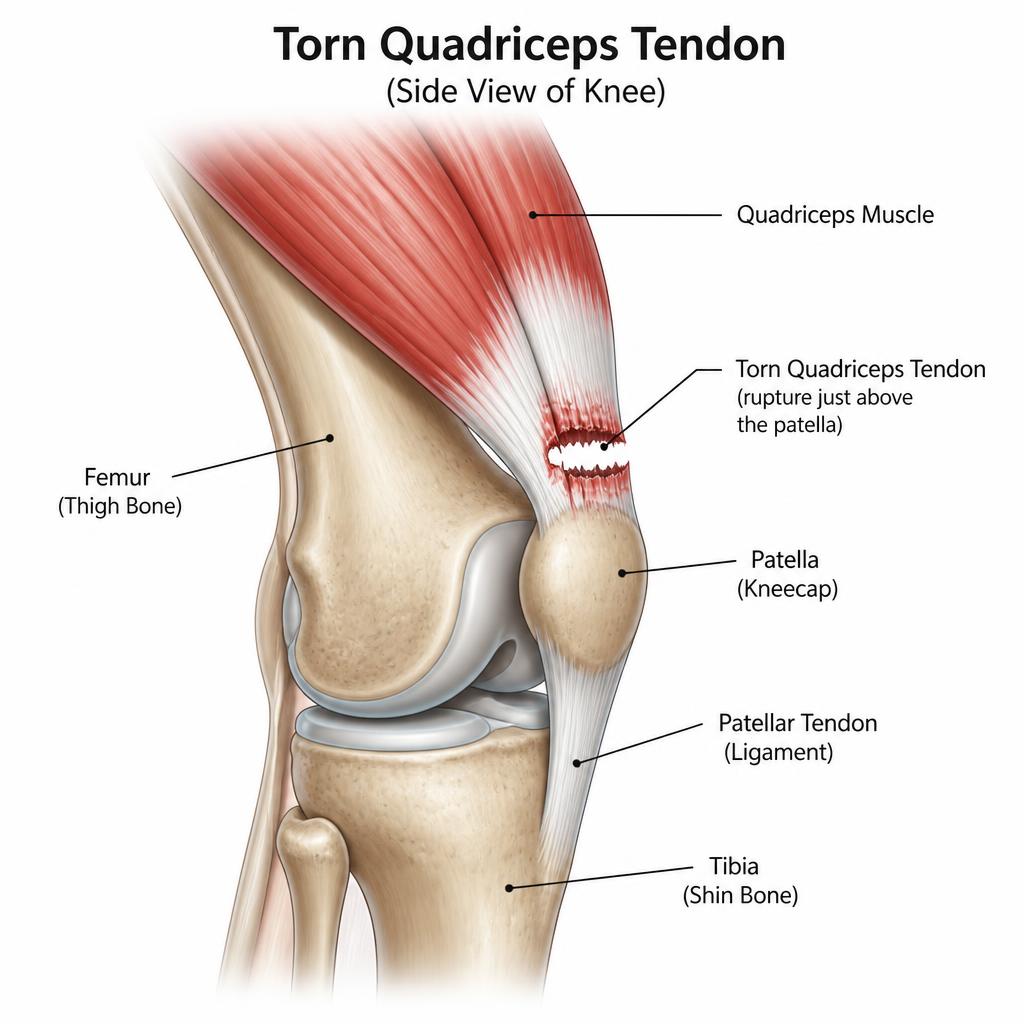
Quadriceps tendon tear
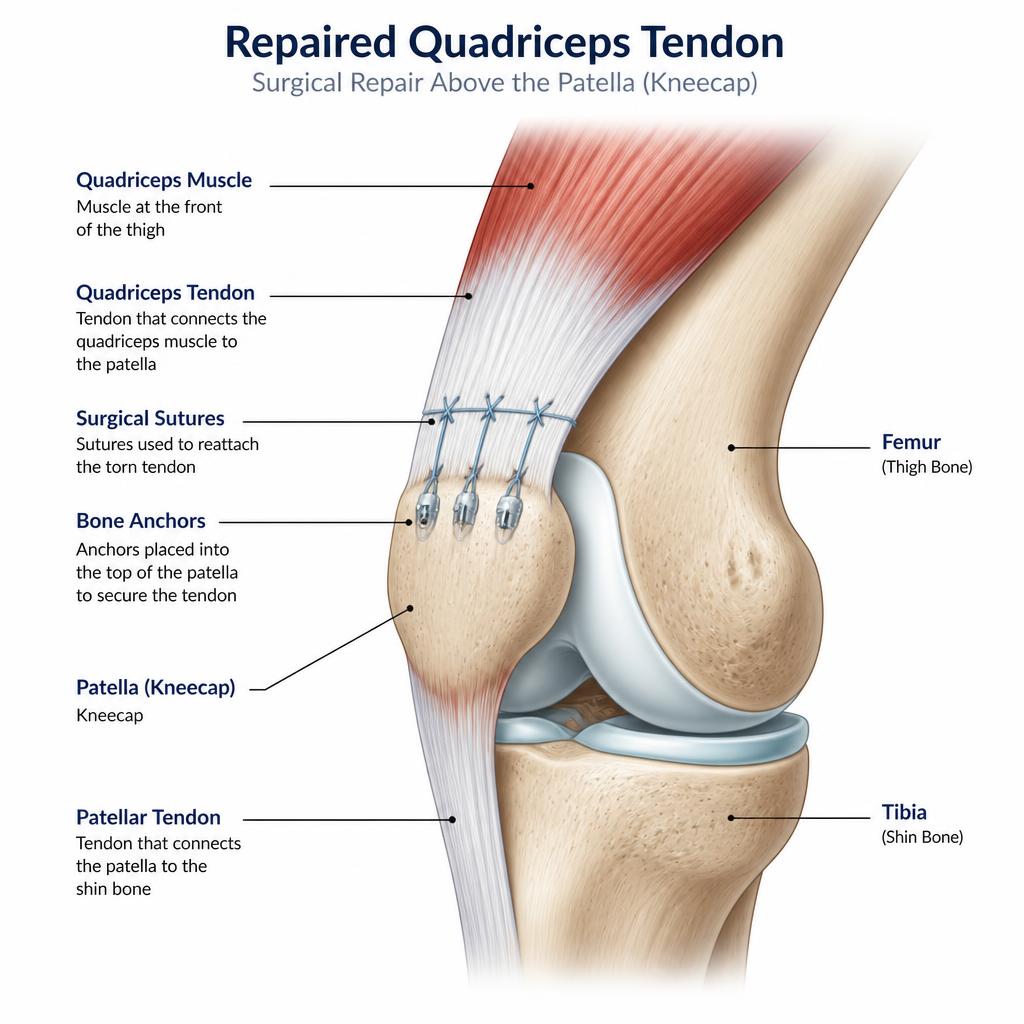
The quadriceps tendon connects the thigh muscle to the top of the kneecap. A rupture here causes the kneecap to drop and the knee gives way when trying to straighten it. The images below show the injured tendon and the tendon after surgical repair.
Surgery
Repair of a ruptured tendon restores the extensor mechanism so you can straighten and control the knee again. The principles of surgery and the main risks are summarised below.
Why surgery is needed
A complete patellar or quadriceps tendon rupture disrupts the extensor mechanism — the system that straightens the knee. Without it you cannot actively straighten the leg or hold the knee against gravity. Surgical repair is almost always recommended, and the best results are achieved when it is performed early, ideally within the first couple of weeks.
Patellar tendon repair
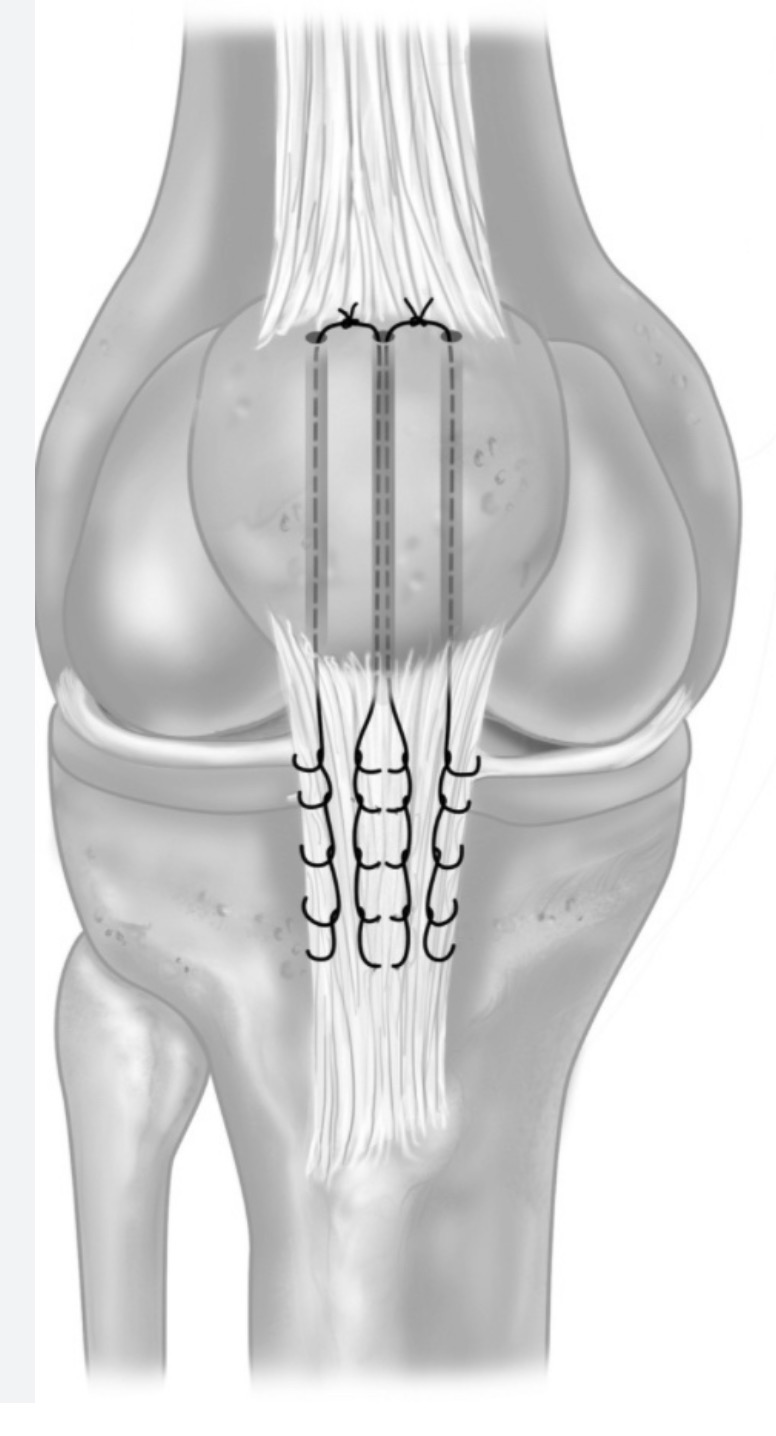
The torn tendon is reattached to the lower pole of the kneecap using strong sutures passed through bone tunnels or secured with suture anchors. The repair restores tendon length and tension so the kneecap sits in its normal position.
Quadriceps tendon repair
The torn quadriceps tendon is reattached to the upper pole of the kneecap with sutures through bone tunnels or anchors. Larger or delayed tears may need reinforcement to protect the repair.
Risks of surgery
As with any operation there are risks, including infection, bleeding, blood clots (DVT/PE), stiffness, weakness, re-rupture, gap formation or lengthening of the tendon, the need for further surgery and scars. These are discussed in full before any decision is made.
Rehabilitation protocol
Variations in rehab protocol can occur based on Mr Rehmatullah’s assessment in theatre.
Recovery is staged to protect the healing tendon while gradually restoring movement, weight bearing and strength. Your individual programme may be adjusted depending on the tear and repair performed.
0–2 weeks
Let the skin heal. Knee held straight in a brace or splint and non weight bearing (NWB) or as advised.
2–6 weeks
Begin gentle physiotherapy with protected range of movement in the brace. Gradually increase weight bearing as guided.
6–12 weeks
Wean off the brace and progress range of movement and weight bearing towards normal walking.
12–24 weeks
Build muscle strength and progress functional and proprioceptive exercises.
12 months
Review in clinic to assess recovery and return to full activity and sport.
Post operatively if you or anyone have concerns about your wound please contact my secretary or myself and do not start any antibiotics unless advised by myself.