Osteochondral Defects
What are osteochondral defects?
An osteochondral defect is an area of damage involving both the cartilage and the bone immediately beneath it. Treated early and appropriately, these lesions can often be repaired or regenerated to preserve the knee and delay or avoid joint replacement.
How they occur
Osteochondral defects can develop suddenly or over time. A single significant injury — such as a twisting injury, dislocation or direct blow to the knee — can shear off a fragment of cartilage and bone. In other patients the cause is osteochondritis dissecans (OCD), where a segment of bone loses its blood supply and the overlying cartilage becomes unstable. Repetitive impact, abnormal joint alignment and previous injury can all contribute.
Symptoms
Symptoms vary with the size and stability of the lesion, but commonly include deep, localised knee pain that is worse with activity, swelling, stiffness and a sense of the knee giving way. If a fragment becomes loose it can cause catching, locking or a blocking sensation as it moves within the joint.
Diagnosis
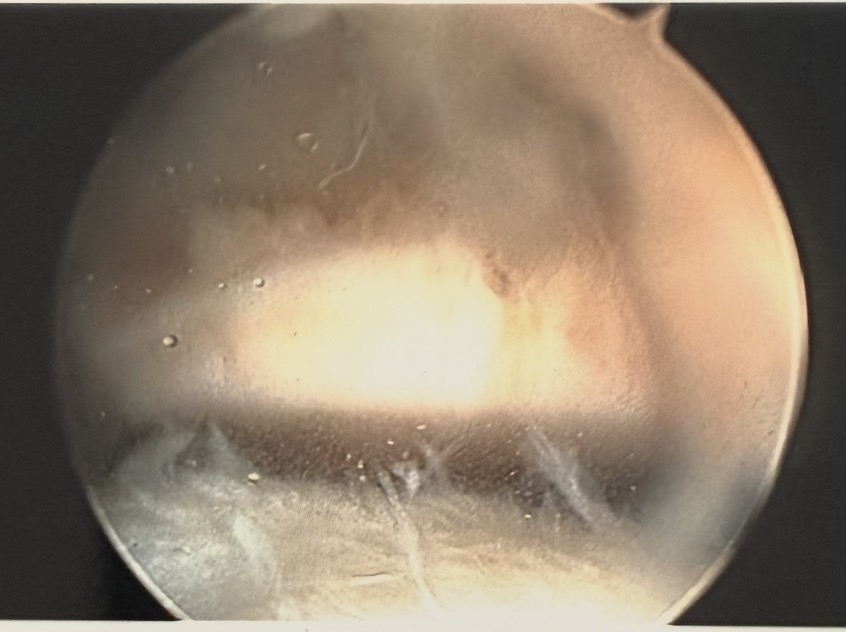
Diagnosis begins with a thorough history and clinical examination. X-rays can show bony involvement and help assess alignment, but MRI is the key investigation — it shows the size, depth and stability of the lesion and the condition of the surrounding cartilage and bone. Occasionally arthroscopy (keyhole surgery) is used to directly assess and grade the defect.
Treatment options
Conservative management
For small, stable lesions — activity modification, physiotherapy, muscle strengthening and load management, sometimes supported by injections to control symptoms.
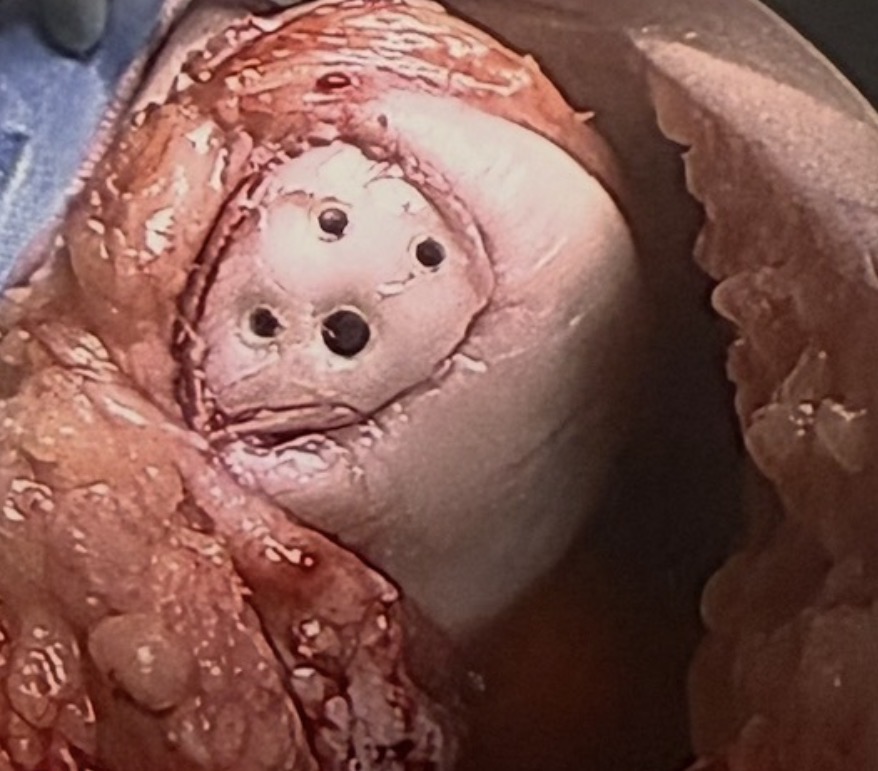
Microfracture
Tiny holes are made in the bone beneath the defect to stimulate a healing response and the formation of fibrocartilage repair tissue. Best suited to smaller defects.
Fixation of the fragment (OCD fixation)
Where a fragment of cartilage and bone has partly detached, it can often be reattached and stabilised with small screws or pins to preserve the native surface.
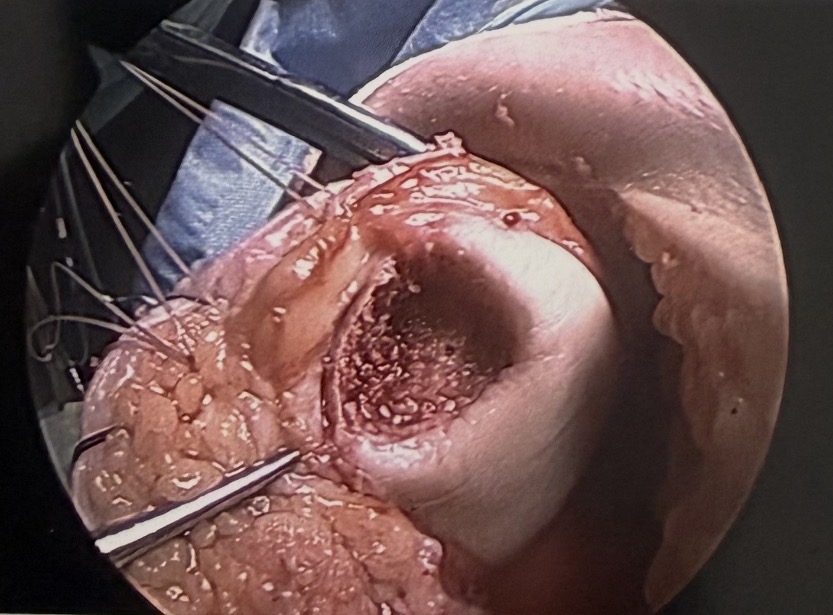
Osteochondral grafting (OATS)
Plugs of healthy cartilage and bone are transferred to fill the defect — using your own tissue (autograft) for smaller lesions or donor tissue (allograft) for larger ones.
Cartilage regeneration (ACI / Spherox)
Cell-based techniques that use your own cultured cartilage cells to regenerate hyaline-like cartilage in larger defects, helping to delay or avoid joint replacement.
Surgery & rehabilitation protocol
Recovery is staged to protect the healing repair while gradually restoring movement, weight bearing and strength. Your individual programme may be adjusted depending on the procedure performed.
0–2 weeks
Let the skin heal. Brace worn at all times and non weight bearing (NWB).
2–6 weeks
Begin physiotherapy. Continue with the brace and remain non weight bearing (NWB).
6–12 weeks
Remove the brace and start gradually weight bearing as guided.
12–24 weeks
Focus on improving muscle strength and progressing function.
12 months
Review in clinic with a repeat MRI to assess healing of the repair.
After surgery if you or anyone have concerns about your wound please contact my secretary or myself and do not start any antibiotics unless advised by myself.